VaidehiPatel
A researcher who builds. An engineer who investigates.
Bachelor's in Computer Engineering taught me to understand systems — how they're built, where they fail, what the architecture is actually doing beneath the surface. A brain injury and four years in medical device manufacturing pulled me toward neuroscience. Master's in Cognitive Neuroscience is where that engineering instinct and personal curiosity finally met the right problem. The combination is rarer than either alone — and it shows up in the work.
across 10 countries
per subject
via parallel batching
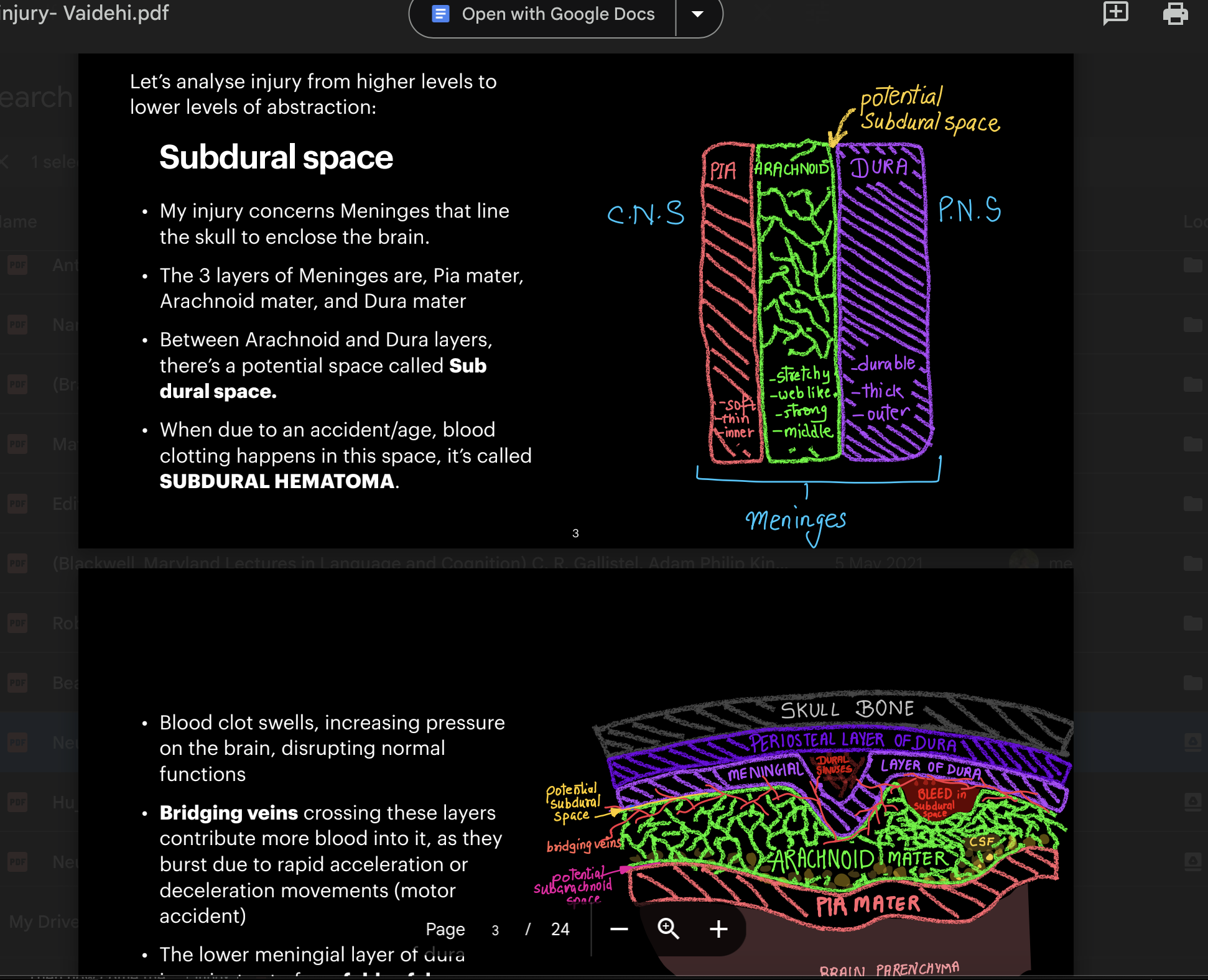
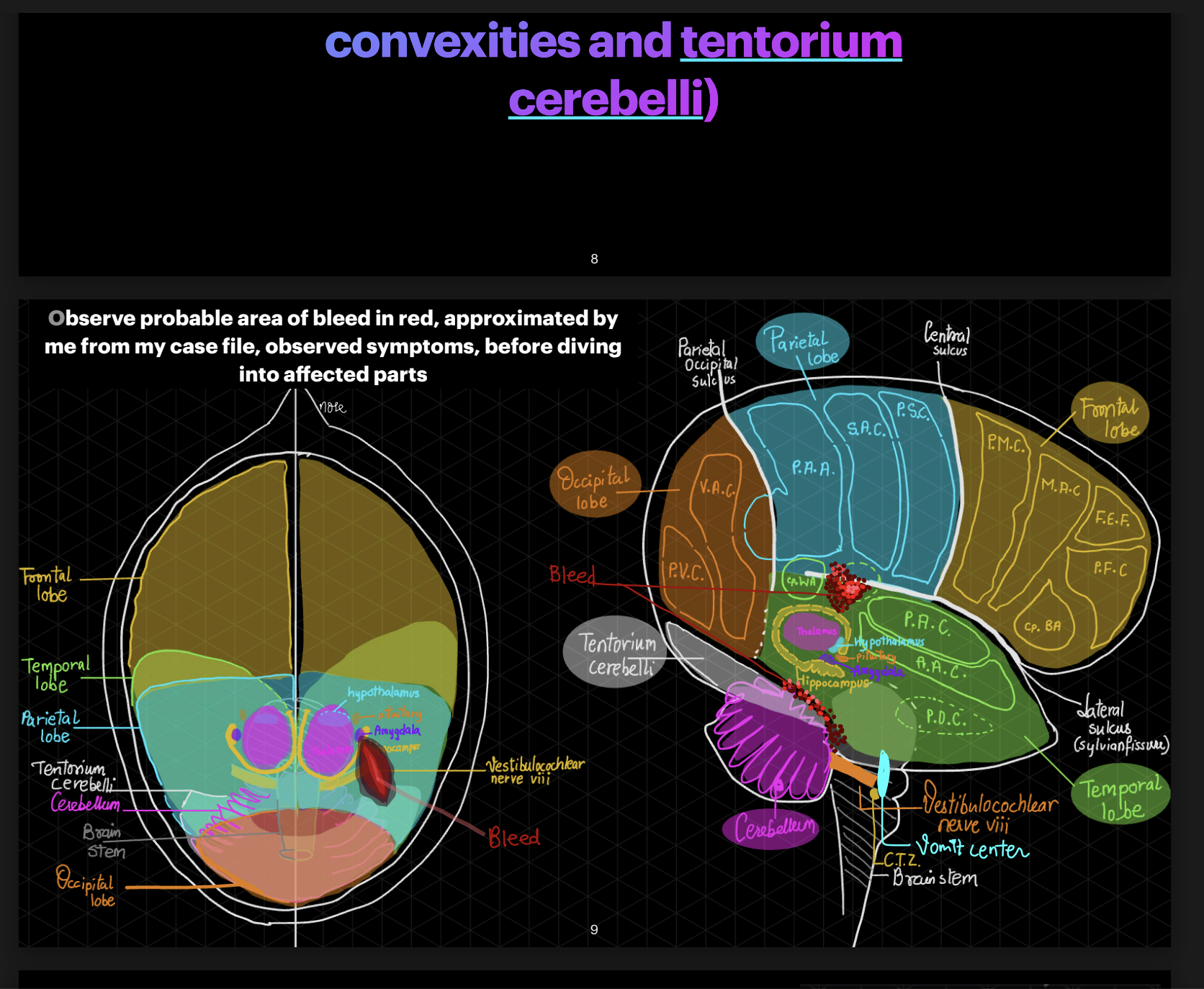
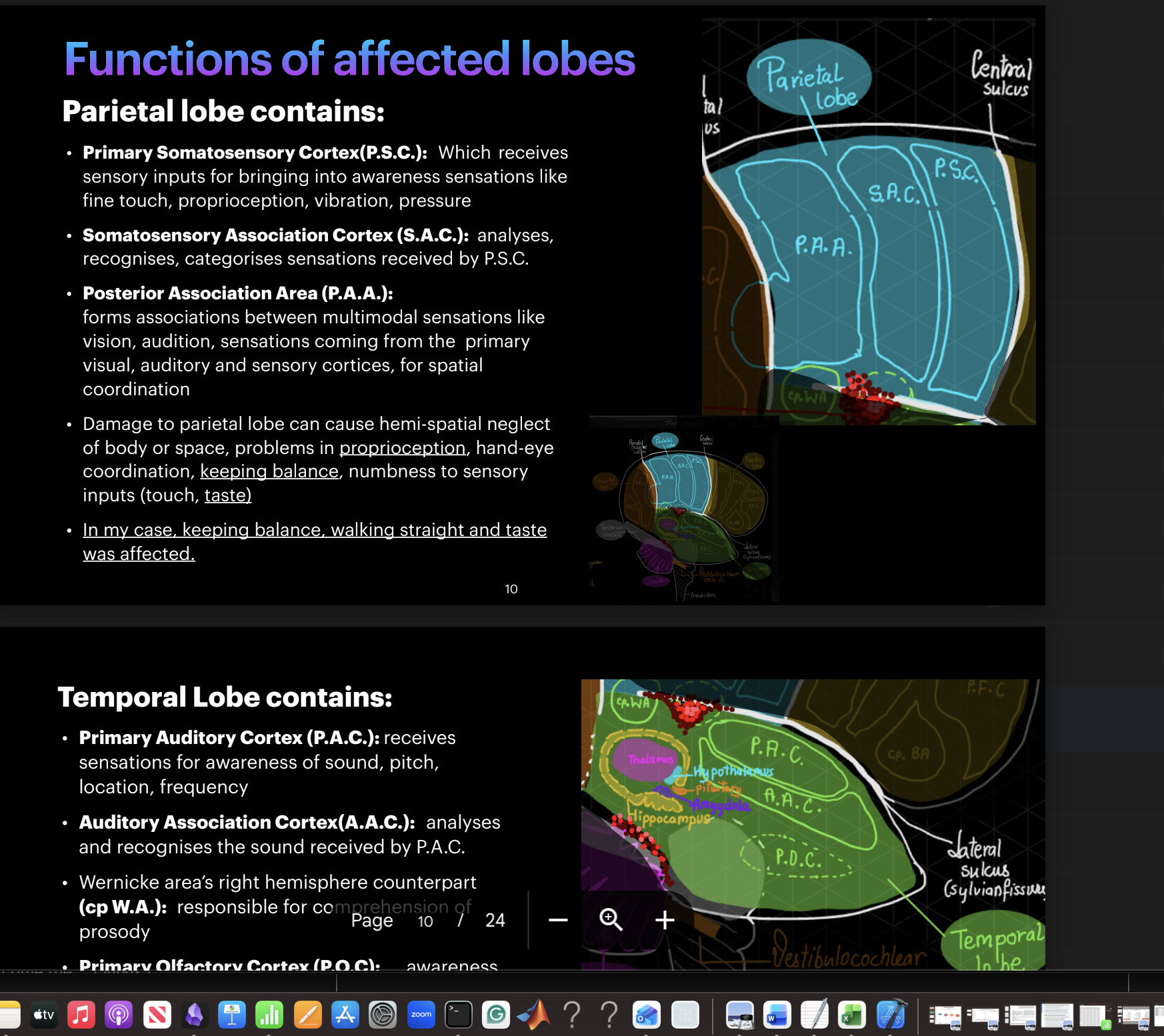
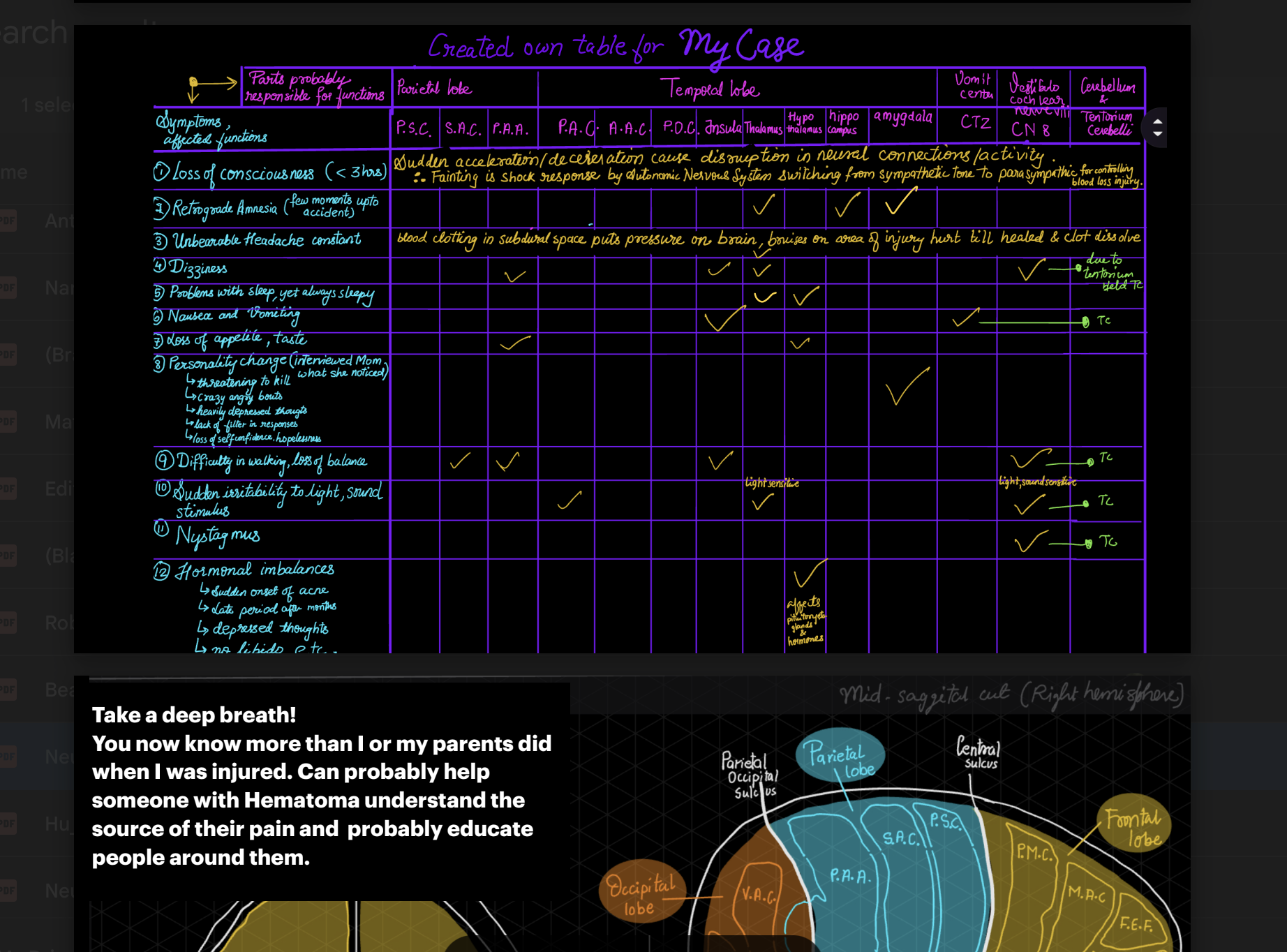
I’m a Computer Engineer turned Neuroscientist. This shift didn’t happen suddenly, but through a slow accumulation of questions I had no framework to answer yet. I was working at a medical device company during COVID-19 when the pandemic stillness gave me time to learn neuroanatomy— finally addressing the questions left over from my own traumatic brain injury a few years prior. I attended online neuroscience conferences and took beginner courses, thinking it was just a phase that would pass once my curiosity was satisfied.
Then, one book changed everything: My Stroke of Insight by Jill Bolte Taylor. It featured a neuroscientist narrating her own stroke— experiencing from the inside what she had only ever studied from the outside. Becoming the observed instead of the observer. Something shifted in how I understood my own injury and recovery. The fuel for my curiosity stopped being "why me" and became something more useful: ensuring that one day, someone else going through something similar doesn't have to feel the way I did.
Mere advocacy and volunteering felt insufficient when my own recovery pointed directly at gaps in how the field understood the injury. The trial-and-error of medications and the sense of being "managed" rather than understood created a frustration that could only be resolved by what I CAN DO for this problem. That drove everything that followed: a mission to transform one of the worst things that happened to me into one of the best things I could do for others.
Clinical recovery may have returned me to a "normal" life, but never to the feeling of being fully restored. I realized full recovery isn’t measured by the clinical absence of impairment, but by the reclamation of one’s potential— the very thing I had abandoned the moment I woke up in the ICU. The space provided by the pandemic finally allowed me the room to grieve that loss and, ultimately, to find a reprieve.
I began seeking out researchers who approached these questions methodically. That path led me to one of the few MS programs in Cognitive Neuroscience in the U.S., where I focused on mapping the brain's neurovascular system after moderate-to-severe TBI. My thesis produced one of the first surface-based CBF-fALFF neurovascular coupling (NVC) analyses in TBI at hemisphere and vertex-neighborhood scales.
As a Research Assistant, I scaled that thesis into a longitudinal, multi-scale NVC analysis. I built an end-to-end pipeline across five nested spatial scales: whole-brain, hemisphere, Yeo-7 networks, DKT atlas regions, and vertex neighborhoods. The investigation grew finer with each scale, answering what the previous one couldn't. A journal manuscript for this work is currently in preparation.
TBI is where I built my proof of work, but it is not the ceiling. Once I understand a system clearly enough to simplify the scales of looking at it, the transferability of skills to problem-solve is inevitable. I am drawn to any hard problem at the intersection of how the brain works and how we build systems to understand or augment it [be it biological, computational, rehabilitative].
This Manuscript/RA work began after my work as graduate research student, with a situation where I was looking at thesis problem statement either too zoomed out or too zoomed in to see with clarity, since the hemisphere or vertex level NVC values indicating significant group differences, didn't tell me where the most NVC disruption exists or if its limited to lesioned areas, whether it follows functional network boundaries, anatomical regions, or something finer. Hence the idea of nested scales of investigation came to mind, starting broad and narrowing until the resolution can't get finer for the computing power available to me. I built end-to-end scripts for each of five scales handling pre-processing, data conversion, lesion masking, NVC calculations, group differences, FDR corrections, visualization of significant results for each.
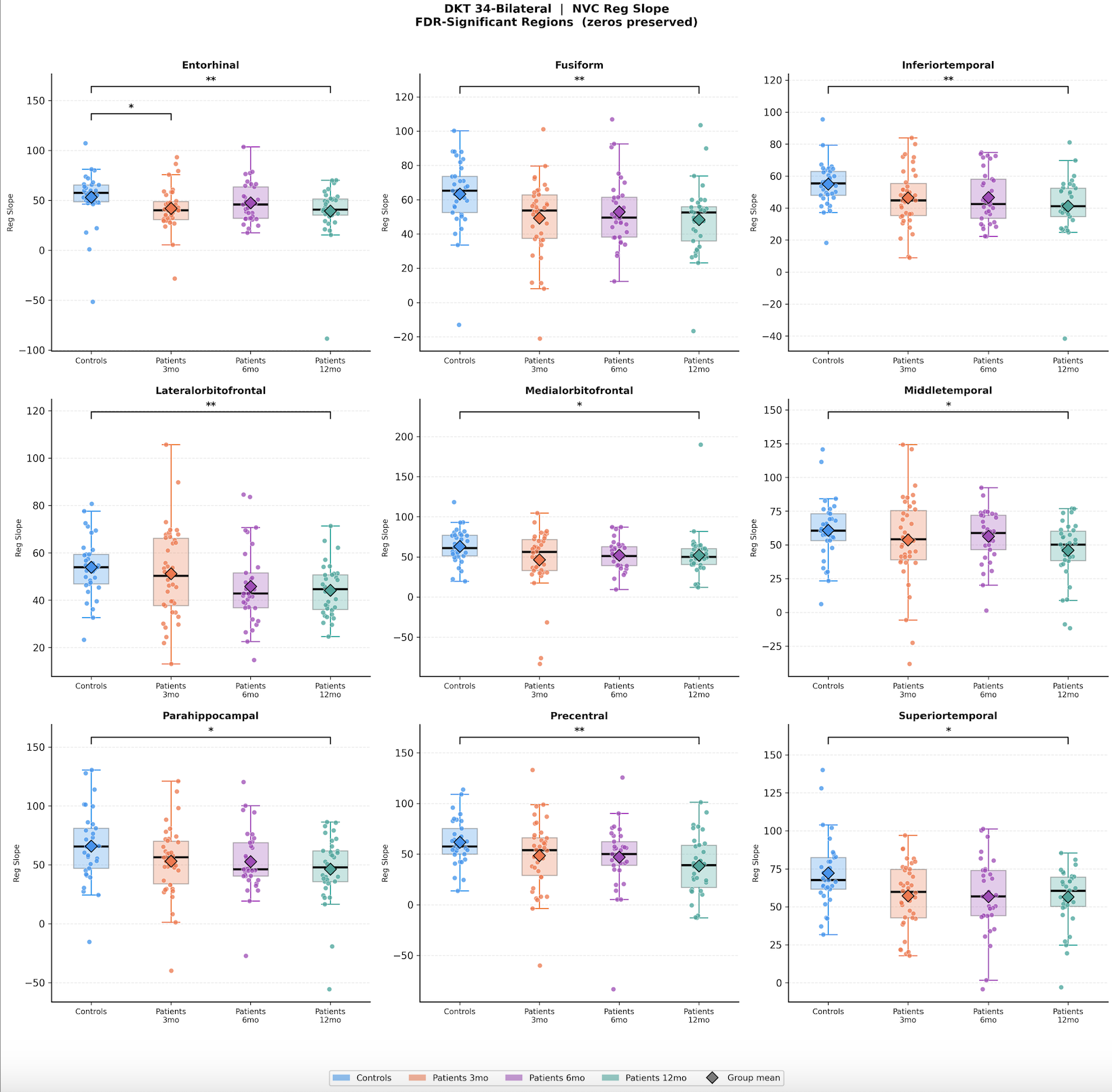
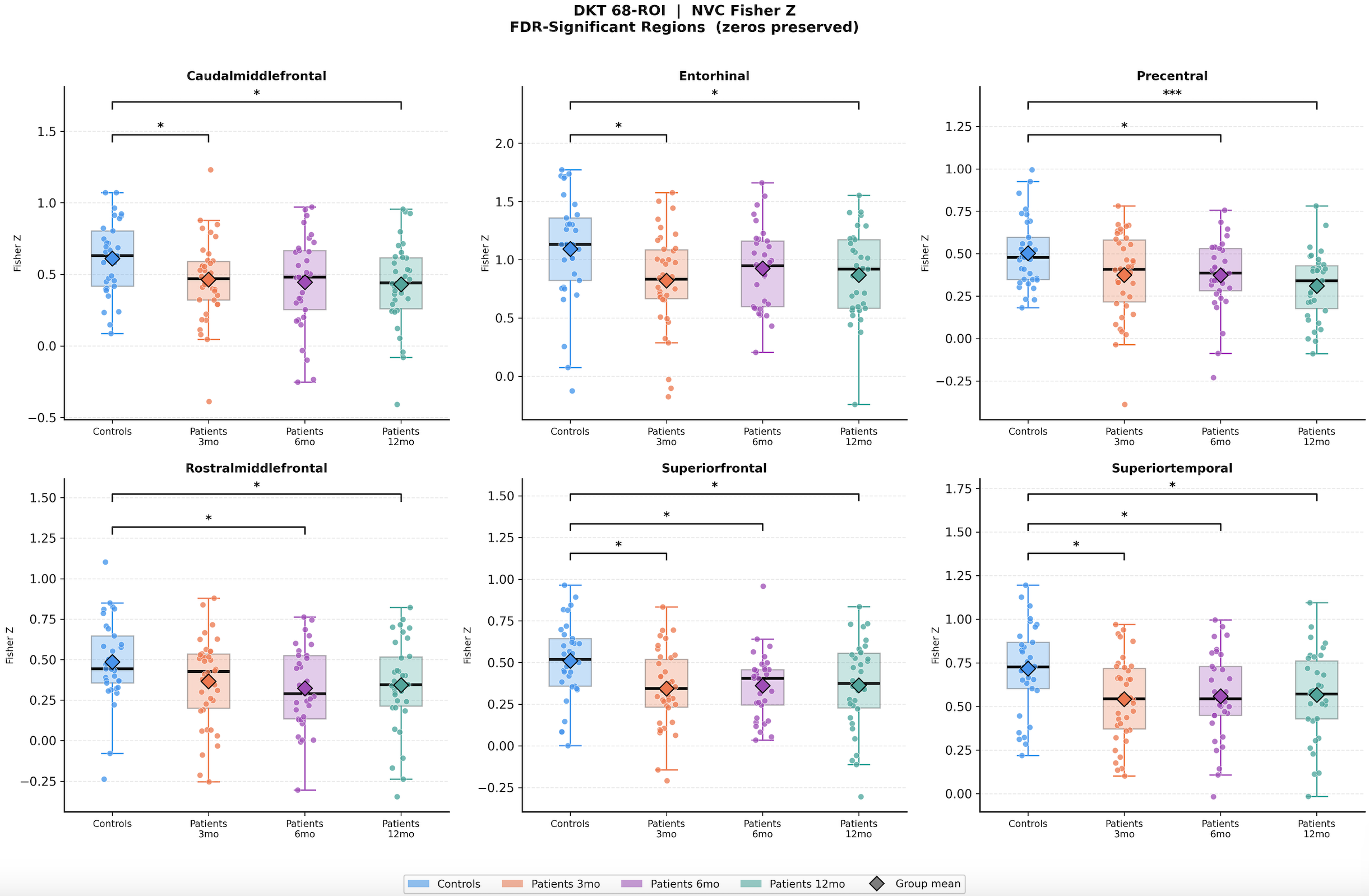
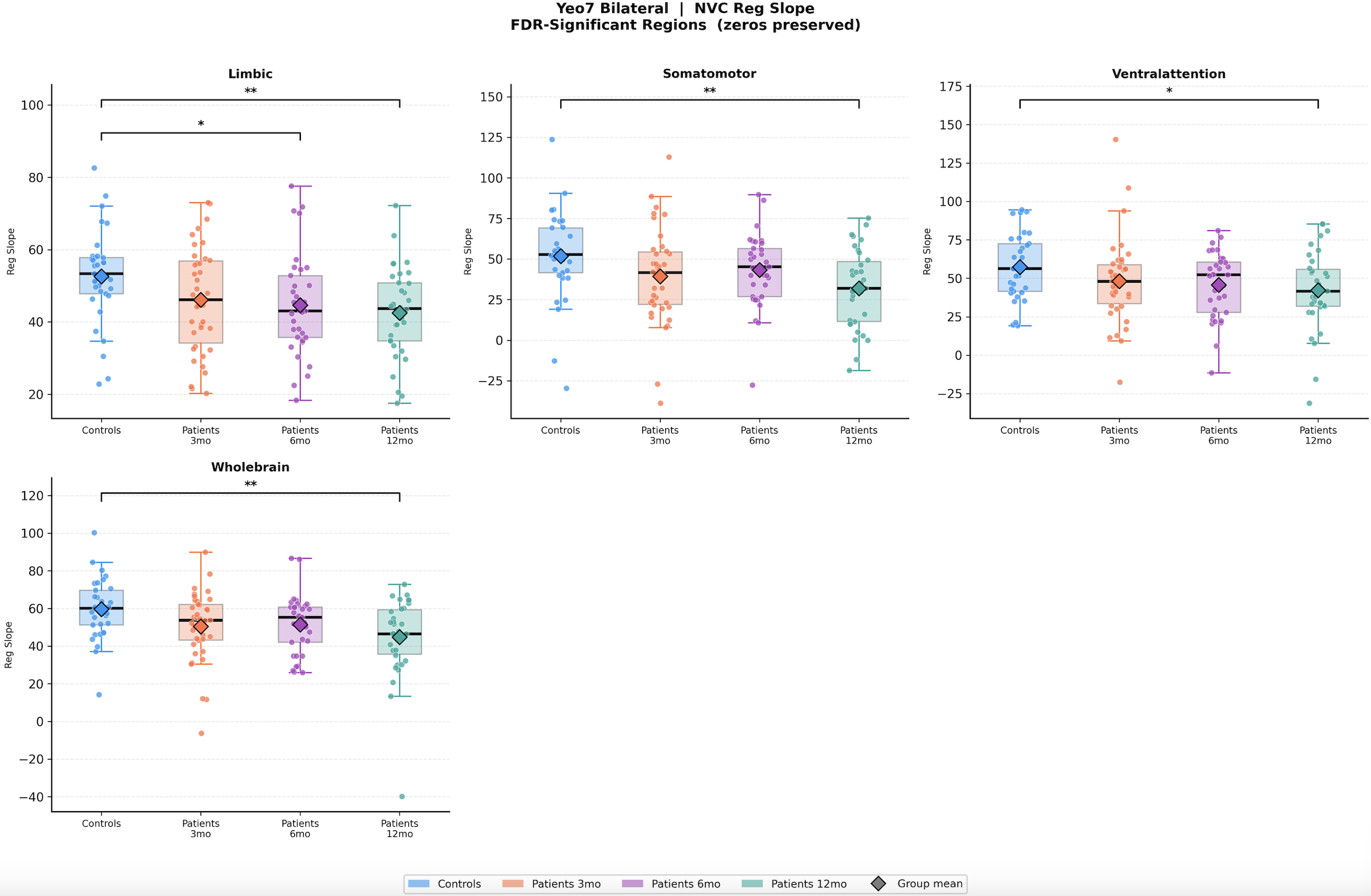
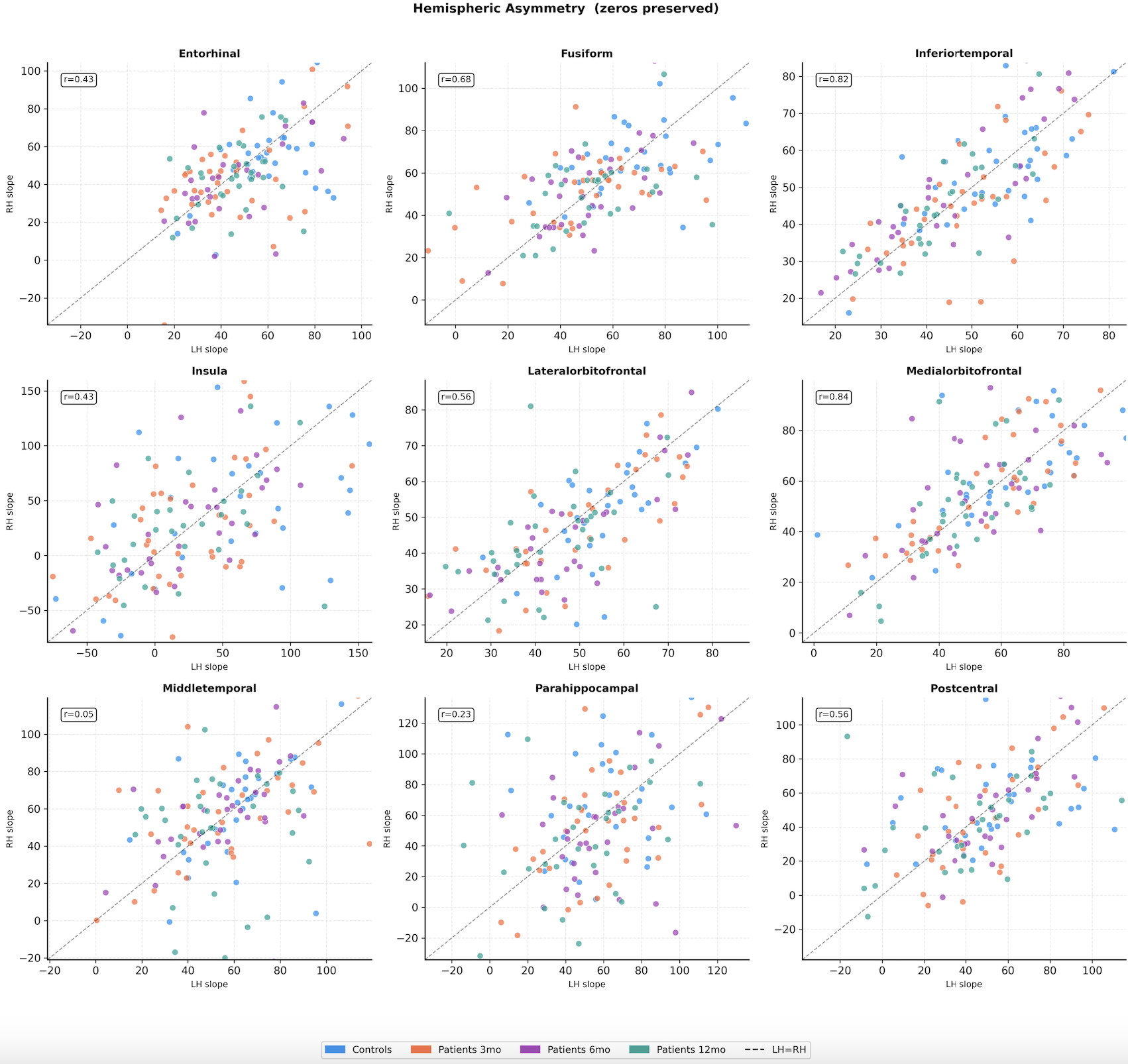
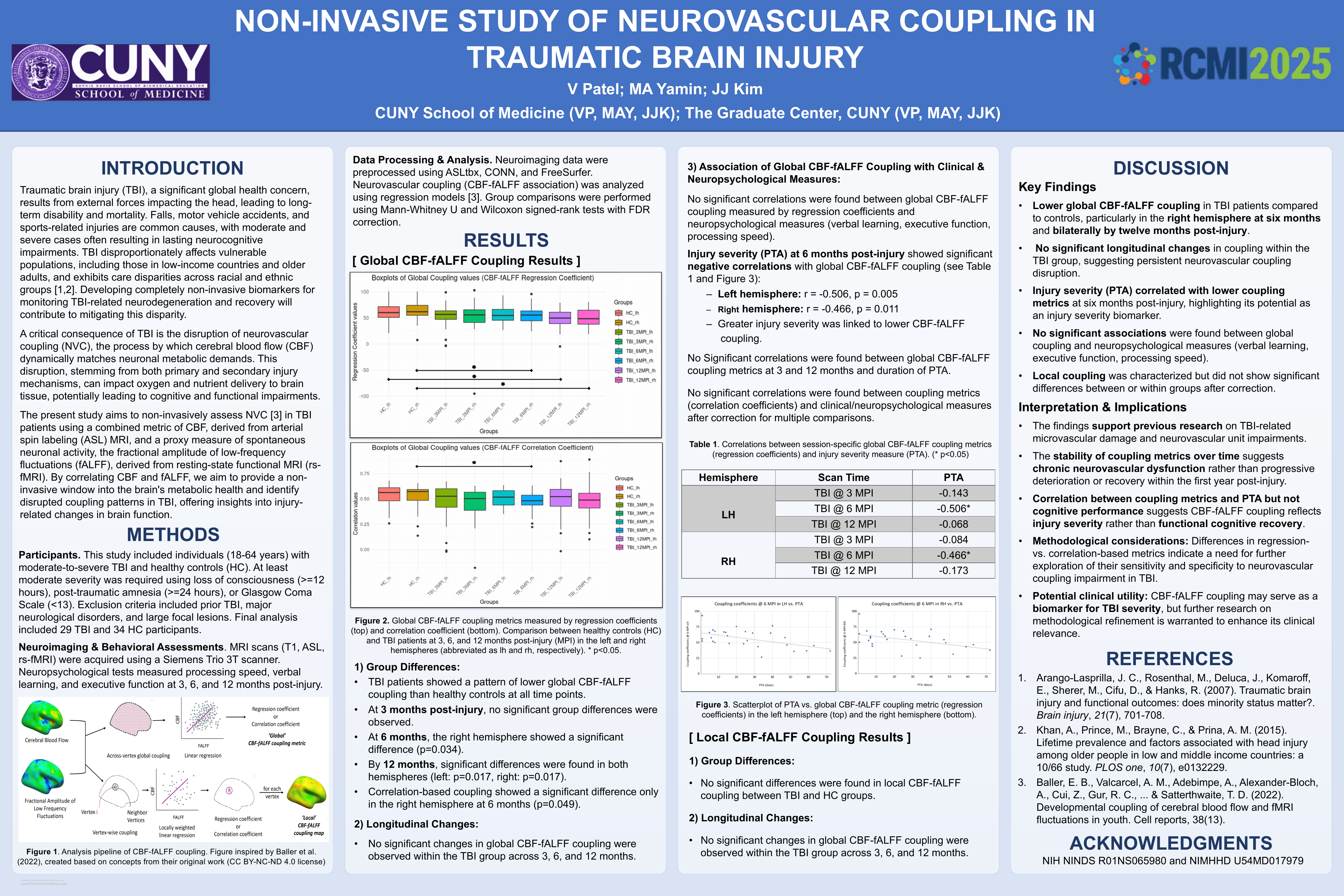
Mapping surface-based neurovascular coupling in moderate-to-severe TBI at hemisphere and vertex neighborhood scales. Found significant group differences bilaterally at 12 months post injury, unilaterally at 6 months post injury and a significant negative correlation with injury severity at 6 months, supporting NVC as a candidate non-invasive biomarker of neurovascular integrity post-TBI
Patel, V. H. (2025). Vertex-based analysis of cerebral blood flow and fractional amplitude of low-frequency fluctuations (CBF-fALFF) coupling in moderate-to-severe traumatic brain injury during the first year post-injury [Master's thesis, The City University of New York]. CUNY Academic Works. https://academicworks.cuny.edu/gc_etds/6138/
The standard ASL pre-processing pipeline had no scrubbing module, and available SCRUB and SCORE tools didn't fully fit our requirements for TBI outlier cohort so I architected and validated a scrubbing module in the pipeline after determining the right point for it in the pre-processing sequence, while accounting for effects on dependent pre-processing steps, intermediate inputs and outputs.
Arterial spin labelling tags water in blood magnetically, lets it flow into brain tissue, subtracts labelled from control to measure cerebral blood flow. No contrast agent. But SNR is low — the signal is ~1% of background. Every source of noise matters.
fMRI scrubs individual corrupted frames. ASL can't — CBF = control − label as a pair. Remove one frame, you corrupt the subtraction. Remove neither, the outlier CBF value contaminates everything downstream, including the NVC coupling calculation it feeds into.
Moderate-to-severe TBI patients move more during scanning. Standard motion thresholds designed for healthy adults or specific pathologies would exclude too much data, for ranges normal in TBI. The pipeline needed parameters that account for the population at the right stage of pre-processing, considering effects on dependent functions, modifications in intermediate inputs and outputs
While inserting the TBI scrubbing stage, a contested assumption surfaced in the lab: does SPM's realignment use the first volume or the mean image as its reference? The answer determined whether motion parameters would shift after volume removal — and whether the pipeline needed to re-run realignment from scratch for subjects. Rather than guessing, I traced through the full call stack with line references: batch_realign.m → spm_realign_asl.m → realign_series() → cleanandsave_parameters().
Conference presentation of the thesis findings — significant bilateral NVC group differences at 12 months post-injury, unilaterally at 6 months and coupling strength negatively correlated with injury severity at 6 months. Co-authored with MA Yamin and JJ Kim. Research funded by NIH NINDS and NIMHHD.
Patel, V., Yamin, M. A., & Kim, J. J. (2025). Non-invasive study of neurovascular coupling in traumatic brain injury [Poster presentation]. RCMI 2025, New York, NY.
CareerOS — Multi-Agent Job Search System
Prototype- in active useCareerOS is a multi-agent job search system I built because I needed to understand my own market value, and systematically reverse engineer the mismatch I felt under a mountain of contradictory advice that no existing platform addressed to my satisfaction. The human gate in this system isn't a limitation — it's the feature that makes everything downstream trustworthy.
It scouts across 70+ job boards, ATS platforms, academic boards, government labs, and direct company careers pages — generating targeted search queries stratified by how recently the role was posted. The fit scorer cites exact phrases from each job description rather than matching keywords; every score is auditable. The eligibility screener classifies employer type using rules the job seeker specifies, even when no policy is mentioned explicitly. Market align feeds the language of liked postings back into the scout layer — the system updates what it searches for based on what the market actually wants.
The fabrication guard runs throughout. Nothing proceeds without human review at the intermediate stage. The goal was never full automation — it was knowing exactly what to delegate.
While working in operations at a medical device manufacturer, I had visibility into the gap between what we were producing and what we needed for FDA clearance, to get that certification to expand our export opportunities. The engineering was rigorous but our regulatory pathway was not clearly mapped being a small company with limited budget and resources to spend on middlemen, consultants to get the certification done systematically. It took me some time but I understood the framework and mapped a plan for making it happen.
A 12-month master plan for FDA 510(k) clearance of a cementless total hip replacement system — three parallel tracks across four quarterly phases. QMS establishment, predicate analysis, biocompatibility strategy, FEA and worst-case selection, mechanical testing, sterilization validation, IFU, packaging, and submission. Each node in the interactive plan contains the applicable standard, SOP, dos and don'ts, and gaps identified from actual device documentation.
The gaps are real. The standards are current. The plan is designed to be handed to a team and executed.
ASLtbx
SPM12
Vertex-wise & ROI analysis
Cortical parcellation
Matplotlib, Nibabel)
R
MATLAB
Bash
FDR correction
Longitudinal analysis
Pipeline design
Multi-agent architecture
Prompt engineering
Agent orchestration
Root cause analysis
Technical documentation
Neuroimaging QA-QC
Experimental design
Mentorship
IRB compliance
Human subjects research
Neuropsychological assessment
Experimental design
